Increase in Fatal Drug Overdoses Across the United States Driven by Synthetic Opioids Before and During the COVID-19 Pandemic

Distributed via the CDC Health Alert Network
December 17, 2020, 8:00 AM ET
CDCHAN-00438
Summary
The purpose of this Health Alert Network (HAN) Advisory is to alert public health departments, healthcare professionals, first responders, harm reduction organizations, laboratories, and medical examiners and coroners to—
(1) substantial increases in drug overdose deaths across the United States, primarily driven by rapid increases in overdose deaths involving synthetic opioids excluding methadone (hereafter referred to as synthetic opioids), likely illicitly manufactured fentanyl;
(2) a concerning acceleration of the increase in drug overdose deaths, with the largest increase recorded from March 2020 to May 2020,coinciding with the implementation of widespread mitigation measures for the COVID-19 pandemic;
(3) the changing geographic distribution of overdose deaths involving synthetic opioids, with the largest percentage increases occurring in states in the western United States;
(4) significant increases in overdose deaths involving psychostimulants with abuse potential (hereafter referred to as psychostimulants) such as methamphetamine; and
(5) recommendations for communities when responding to the evolving overdose crisis.
Background
The most recent provisional data available from the Centers for Disease Control and Prevention’s (CDC) National Center for Health Statistics (NCHS) indicate that approximately 81,230 drug overdose deaths occurred in the United States in the 12-months ending in May 2020 (Figure 1).i This represents a worsening of the drug overdose epidemic in the United States and is the largest number of drug overdoses for a 12-month period ever recorded.1 After declining 4.1% from 2017 to 2018,2 the number of overdose deaths increased 18.2% from the 12-months ending in June 2019ii to the 12-months ending in May 2020 (Figure 1).3 Drug overdose deaths during this time increased more than 20% in 25 states and the District of Columbia, 10% to 19% in 11 states and New York City, and 0% to 9% in 10 states. Drug overdose deaths decreased in four states (Figure 2).
The recent increase in drug overdose mortality began in 2019 and continues into 2020, prior to the declaration of the COVID-19 National Emergency in the United States in March. The increases in drug overdose deaths appear to have accelerated during the COVID-19 pandemic. Provisional overdose death estimates indicate that the largest monthly increases in drug overdose deaths occurred in the 12-months ending in February 2020 (74,185 deaths) and the 12-months ending in March 2020 (75,696 deaths), the 12-months ending in March 2020 (75,696 deaths) to the 12-months ending in April 2020 (77,842 deaths), and from the 12-months ending in April 2020 (77,842 deaths) to the 12-months ending in May 2020 (81,230 deaths). These one-month increases of 2,146 deaths and 3,388 deaths, respectively for the 12-month periods (Figure 1), are the largest monthly increases documented since provisional 12-month estimates began to be calculated in January 2015.3
Synthetic opioids are the primary driver of the increases in overdose deaths. The 12-month count of synthetic opioid deaths increased 38.4% from the 12-months ending in June 2019 compared with the 12-months ending in May 2020 (Figure 1). Of the 38 jurisdictions with available synthetic opioid data,3 37 jurisdictions reported increases in synthetic opioid overdose deaths for this time period. Eighteen of these jurisdictions reported increases greater than 50%, 11 reported increases of 25% to 49%, 7 reported increases of 10% to 24%, 1 reported an increase <10% (See Figure 3). State and local health department reports indicate that the increase in synthetic opioid-involved overdoses is primarily linked to illicitly manufactured fentanyl.4-6 Historically, deaths involving illicitly manufactured fentanyl have been concentrated in the 28 states east of the Mississippi River, where the heroin market has primarily been dominated by white powder heroin.5,7 In contrast, the largest increases in synthetic opioid deaths from the 12-months ending in June 2019 to the 12-months ending in May 2020 occurred in 10 western states (98.0% increase).iii This is consistent with large increases in illicitly manufactured fentanyl availability in western states8 and increases in fentanyl positivity in clinical toxicology drugs tests in the West after the COVID-19 pandemic.9 Increases in synthetic opioid overdose deaths were also substantial in other regions: 12 southern states and the District of Columbia (35.4%), 6 midwestern states (32.1%), and 8 northeastern states and New York City (21.1%) (Figure 3).
Overdose deaths involving cocaine also increased by 26.5% from the 12-months ending in June 2019 to the 12-months ending in May 2020 (Figure 1). Other data have shown that recent increases in overdose deaths involving cocaine are primarily related to overdose deaths that involved both cocaine and synthetic opioids (primarily illicitly manufactured fentanyl).10 These deaths are likely linked to co-use of cocaine among people injecting opioids such as illicitly manufactured fentanyl or heroin.11 In contrast, overdose deaths involving psychostimulants, such as methamphetamine, have been increasing with and without synthetic opioid co-use and at a rate faster than overdose deaths involving cocaine.10 Provisional 12-month counts of overdose deaths involving psychostimulants in the United States increased by 34.8% from the 12-months ending in June 2019 compared to the 12-months ending in May 2020. The number of deaths involving psychostimulants now exceeds the number of cocaine-involved deaths (Figure 1). These increases are consistent with the increased availability of methamphetamine in the illicit drug supply and increases in methamphetamine-related treatment admissions.8,12-14
Recommendations
These newly released provisional fatal overdose data, coupled with the known disruption to public health, healthcare, and social services as a result of the COVID-19 pandemic and related mitigation measures, highlight the need for essential services to remain accessible for those most at risk of overdose and the need to expand prevention and response activities. CDC recommends the following actions as appropriate based on community needs and characteristics:
- Expand the provision and use of naloxone and overdose prevention education
- Public health departments and community-based organizations:
- Raise awareness about
1) The critical need for bystanders to have naloxone on hand and use it during an overdose;
2) The changing illicit drug marketplace and the wider availability and geographic dispersion of illicitly manufactured fentanyl and novel psychoactive substances (e.g., fentanyl analogs);
3) Common co-use of illicitly manufactured fentanyl with other drugs such as cocaine and methamphetamine; and
4) Infrequent mixing of illicitly manufactured fentanyl into the illicit drug supplies of methamphetamine and cocaine.7,12 - Increase awareness about the risk of using drugs when alone and emphasize the need for risk reduction strategies among people who use drugs, including during the COVID-19 pandemic. Strategies can include
- Not using drugs alone and knowing what drugs are being used;
- Ensuring naloxone is available and that people who use drugs and their loved ones know how to administer it; and
- Having a friend or loved one check in on people who use drugs regularly, especially during use.
- Provide messaging to community groups (particularly those providing services to high risk populations), community leaders, school officials, faith based leaders, parents, students and others about the changing illicit drug supply and risks for overdose and exposure to highly potent opioids such as illicitly manufactured fentanyl or counterfeit drugs appearing to be legal prescription medications.
- Raise awareness about
- Healthcare providers:
- Talk to patients about the changing illicit drug supply and risks for overdose and exposure to highly potent opioids such as illicitly manufactured fentanyl.
- Prescribe naloxone to individuals at risk for opioid overdose, such as those with a prior history of overdose, those with opioid use disorder, and individuals using illicit opioids and other drugs that might be mixed with illicitly manufactured fentanyl.
- Co-prescribe naloxone to patients with high morphine milligram equivalents and those receiving opioids and benzodiazepines.15
- Expand locations in which overdose prevention education and take-home naloxone are provided. These locations can include inpatient and outpatient treatment programs, primary care settings, retail pharmacies, counseling and support groups, and other community-based settings. Expanding locations may be especially important in rural areas.16-18
- Counsel patients that multiple doses of naloxone may be needed for a single overdose event because of the potency of illicitly manufactured fentanyl and fentanyl analogs,19 and that multiple doses of naloxone may be needed over time due to prolonged effects of opioids in some cases.5,20
- Harm reduction organizations:
- Increase the provision of overdose prevention education and take-home naloxone to people who use drugs, their friends, and others likely to witness or experience an overdose.7,21-23
- Ensure that individuals have sufficient doses of take-home naloxone to account for the potency of illicitly manufactured fentanyl and fentanyl analogs.24
- Call 911 immediately after recognizing an overdose or resuscitating a patient. Naloxone available in the field may not be sufficient to reverse the overdose. Those who receive naloxone may experience a recurrence of overdose symptoms or experience other acute medical, traumatic, toxicologic, or psychiatric conditions.25,26
- Prioritize naloxone distribution to people who use drugs following periods of abstinence and during transitions where opioid tolerance may have waned. There is a higher risk of overdose during these periods, including post-incarceration and after treatment for an opioid use disorder, if a relapse occurs.27,28
- First responders to overdoses:
- Increase the amount of naloxone on hand given the increased amount needed and rate of use for overdoses involving illicitly manufactured fentanyl and fentanyl analogs.29
- Implement and improve post-overdose outreach and follow-up via peer recovery support specialists to promote engagement in treatment.
- Take steps to reduce the risk of COVID-19 exposure when responding to a suspected drug overdose and administering naloxone. These steps include using personal protective equipment (PPE) and positioning the person’s head facing away from you when administering naloxone.
- Public health departments and community-based organizations:
- Expand access to and provision of treatment for substance use disorders
- Healthcare providers:
-
- Provide Medications for Opioid Use Disorder (MOUD)
- Treatment with the FDA-approved medications methadone, buprenorphine, or naltrexone are lifesaving and the most effective forms of treatment for opioid use disorder.
- Ensure treatment access, especially for people who are transitioning from institutional settings such as the criminal justice system, residential treatment, or a recent hospitalization.7,30
- During the COVID-19 public health emergency, the Federal Government has made it easier to obtain MOUD through telehealth.31-33
- Find treatment options or call 1-800-662-HELP (4357).
- SAMHSA’s Buprenorphine Practitioner Locator can help identify a qualified practitioner who can prescribe buprenorphine.
- Provide Stimulant (Cocaine, Methamphetamine) Use Disorder Treatment
- Unlike opioid use disorder treatment, there are no FDA-approved medications to treat stimulant use disorders.
- The most effective treatments for stimulant use disorders are psychosocial therapies such as motivational interviewing, contingency management, contingency management combined with community reinforcement approach, and contingency management combined with cognitive-behavioral therapy. These therapies have demonstrated effectiveness for stimulant use disorders. For additional information about each of these treatment strategies, see SAMHSA’s Treatment for Stimulant Use Disorders.
- Find treatment options or call 1-800-662-HELP (4357).
- Provide Medications for Opioid Use Disorder (MOUD)
- Harm reduction organizations:
- Offer buprenorphine on-site, in a mobile van, or through telemedicine for clients with opioid use disorder.34-36
- Intervene early with individuals at the highest risk for overdose
- Public health departments and harm reduction organizations:
- Link people who are at risk for overdose with care and track their retention in care programs. People who are at risk include those who have recently been treated for a non-fatal overdose.37,38
- Consider expanding peer navigator programs or using recovery coaches to intervene with individuals at the highest risk of overdose.39
- Healthcare providers:
- Initiate or continue medications for opioid use disorder among people leaving correctional and detention facilities. See Recommendation #2 on treatment.
- Provide active referral-to-treatment options and recovery support services.40
- Implement post-overdose response protocols, including in emergency departments, that incorporate links between public health, treatment providers, community-based service organizations, and healthcare providers. These protocols promote overdose education, treatment, linkage to care and MOUD, and naloxone distribution.41,42
- Public safety:
- Divert individuals with low-level drug offenses pending prosecution to case management and supportive wrap-around services instead of jail or prison and prosecution. Diversion enables long-term treatment and recovery.43,44 Examples of diversion programs include Police Assisted Addiction and Recovery Initiative (PAARI) and Law Enforcement Assisted Diversion (LEAD).
- Public health departments and harm reduction organizations:
- Improve detection of overdose outbreaks due to fentanyl, novel psychoactive substances (e.g., fentanyl analogs), or other drugs to facilitate an effective response
- Public health departments:
-
- Identify drug overdose outbreaks and spikes rapidly using existing surveillance systems such as syndromic surveillance emergency department data, emergency medical services data, commercial laboratory data, poison center data, medical examiner or coroner data, and tools like Overdose Detection – Mapping Application Program (ODMAP). Existing syndromic surveillance emergency department data sources include CDC’s Drug Overdose Surveillance and Epidemiology (DOSE) system and the National Syndromic Surveillance Program (NSSP).7,9,45,46
- Track and monitor trends in the illicit opioid drug supply and overdoses, using local, state, and federal data systems and toxicological testing, including:
- The geographic distribution of illicit drugs and overdoses;
- Shifts in demographic characteristics of individuals at risk for overdose (e.g., by sex, race/ethnicity); and
- The identification of the drugs with which opioids are mixed and drug products containing multiple opioids (e.g., heroin and illicitly manufactured fentanyl).
- Medical examiners and coroners:
- Screen specimens, including in suspected overdose deaths involving heroin, using an enzyme-linked immunosorbent assay (ELISA) test that can detect substances including fentanyl and fentanyl analogs.47 See laboratory section below.
- Screen for novel psychoactive substances prevalent in your region or when an unexplained increase in drug overdoses occurs.48
- Consider specialized testing for fentanyl analogs or other novel synthetic opioids when fentanyl screening is negative, or confirmatory testing is inconclusive, yet opioid or fentanyl overdose is highly suspected. This is particularly important if an increase in overdoses is occurring or fentanyl analogs have been detected in local drug products.49
- Laboratories:
- Implement an opioid biosurveillance program in line with the Association of Public Health Laboratories (APHL) guidance on developing model surveillance systems for use in tracking non-fatal opioid overdoses at the state level.
- Use CDC’s Traceable Opioid Material® Kits (TOM Kits®). This product line provides reference materials enabling labs to screen for more than 210 synthetic opioid compounds – including more than 190 fentanyl analogs.50 Available kits include the Opioid Certified Reference Material kit (Opioid CRM kit) and the Fentanyl Analog Screening (FAS) Kit.
- Harm reduction organizations:
- Implement drug checking services and drug supply surveillance in line with applicable state and local laws.51
- Partner with public safety and public health to obtain and disseminate the latest information on local drug supply and overdose trends.51,52
Figure 1: Twelve-month provisionala drug overdose death counts for all drugsb, synthetic opioidsc, cocained, and psychostimulantse, for 50 states, the District of Columbia, and New York City: 12-months ending in June 2019 to 12-months ending in May 2020f
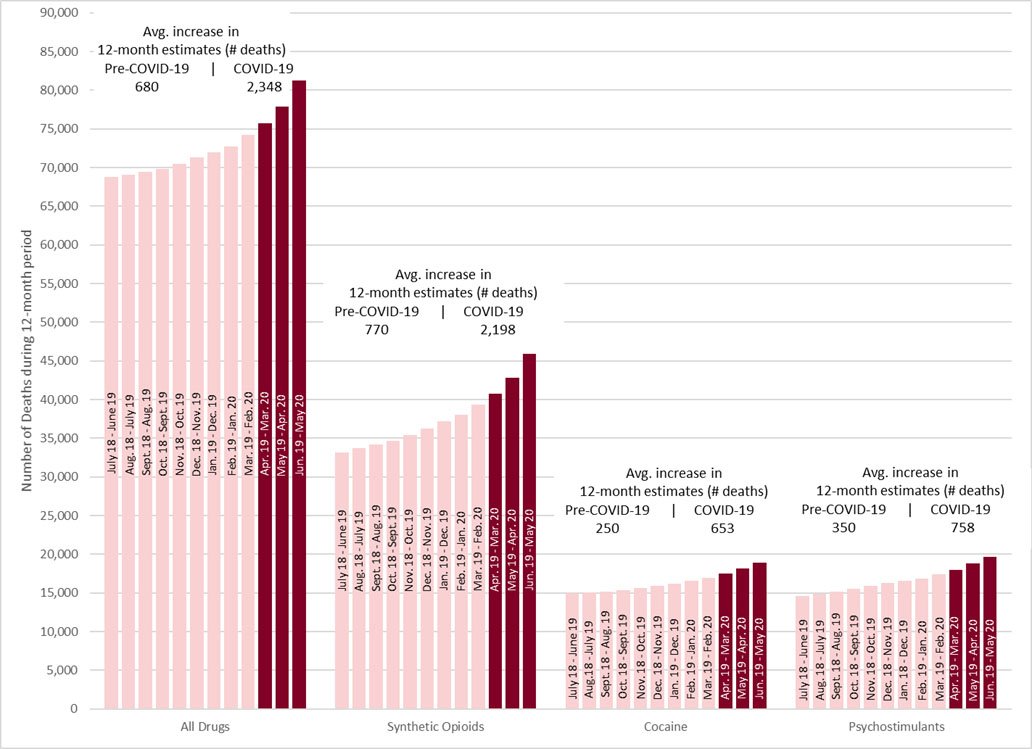
a Provisional drug overdose death counts are based on death records received and processed by NCHS. Provisional drug overdose death data are often incomplete, and the degree of completeness varies by jurisdiction and 12-month ending period. Consequently, the numbers of drug overdose deaths are underestimated based on provisional data relative to final data and are subject to random variation. Provisional data are based on available records that meet certain data quality criteria at the time of analysis and may not include all deaths that occurred during a given time period. Therefore, they should not be considered comparable with final data and are subject to change. The counts used in this analysis are the “predicted” values. Predicted provisional counts represent estimates of the number of deaths adjusted for incomplete reporting.
b Deaths were classified using the International Classification of Diseases, Tenth Revision (ICD–10). Drug overdose deaths were identified using underlying cause-of-death codes X40–X44, X60–X64, X85, and Y10–Y14. The drug classes are all nested within all drug overdose deaths, but multiple drug classes may be involved in a single drug overdose death.
c Drug overdose deaths, as defined, that involve synthetic opioids other than methadone (T40.4).
d Drug overdose deaths, as defined, that involve cocaine (T40.5).
e Drug overdose deaths, as defined, that involved psychostimulants with abuse potential (T43.6).
f Included time periods will have some amount of overlap. For example, the 12-months ending in June 2019 (i.e., July 2018 to June 2019) includes deaths occurring in June 2019, which is also included separately in 12-months ending in May 2020 (i.e., June 2019 to May 2020).
Figure 2: Percentage change in 12-months ending provisionala data on all fatal drug overdosesb, 50 states, the District of Columbia, and New York City: Overdose deaths from 12-months ending in June 2019 to 12-months ending in May 2020c
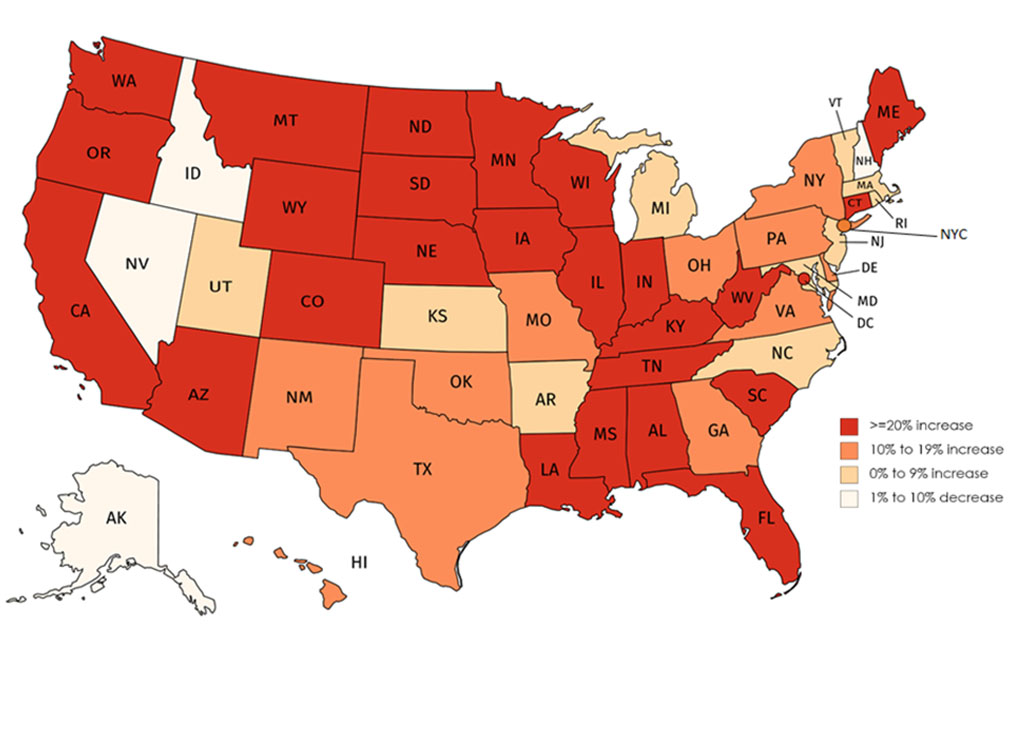
a Provisional drug overdose death counts are based on death records received and processed by NCHS. Provisional drug overdose death data are often incomplete, and the degree of completeness varies by jurisdiction and 12-month ending period. Consequently, the numbers of drug overdose deaths are underestimated based on provisional data relative to final data and are subject to random variation. Provisional data are based on available records that meet certain data quality criteria at the time of analysis and may not include all deaths that occurred during a given time period. Therefore, they should not be considered comparable with final data and are subject to change. The counts used in this analysis are the “predicted” values. Predicted provisional counts represent estimates of the number of deaths adjusted for incomplete reporting.
b Deaths were classified using the International Classification of Diseases, Tenth Revision (ICD–10). Drug overdose deaths were identified using underlying cause-of-death codes X40–X44, X60–X64, X85, and Y10–Y14.
c Included time periods will have some amount of overlap. For example, the 12-months ending in June 2019 (i.e., July 2018 to June 2019) includes deaths occurring in June 2019, which is also included separately in 12-months ending in May 2020 (i.e., June 2019 to May 2020).
Figure 3: Percentage change in 12-months ending provisionala count of fatal overdoses involving synthetic opioidsb, 36 states, the District of Columbia, and New York Cityc: Deaths from 12-months ending in June 2019 to 12-months ending in May 2020d
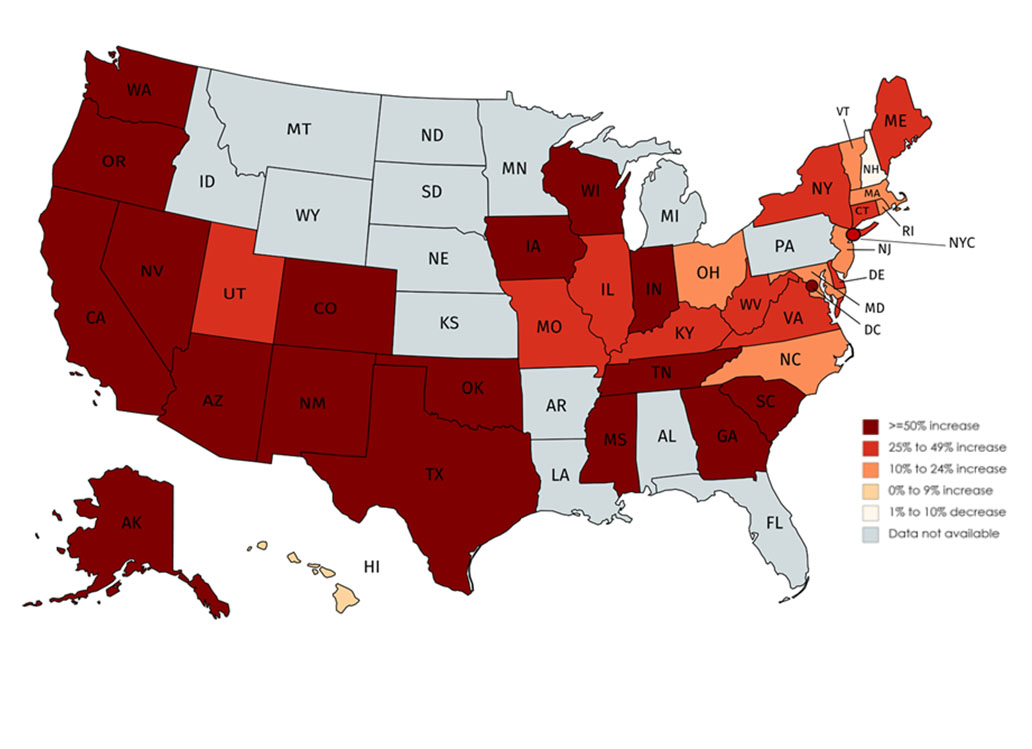
a Provisional drug overdose death counts are based on death records received and processed by NCHS. Provisional drug overdose death data are often incomplete, and the degree of completeness varies by jurisdiction and 12-month ending period. Consequently, the numbers of drug overdose deaths are underestimated based on provisional data relative to final data and are subject to random variation. Provisional data are based on available records that meet certain data quality criteria at the time of analysis and may not include all deaths that occurred during a given time period. Therefore, they should not be considered comparable with final data and are subject to change. The counts used in this analysis are the “predicted” values. Predicted provisional counts represent estimates of the number of deaths adjusted for incomplete reporting.
b Deaths were classified using the International Classification of Diseases, Tenth Revision (ICD–10). Drug overdose deaths were identified using underlying cause-of-death codes X40–X44, X60–X64, X85, and Y10–Y14. Drug overdose deaths, as defined, that involve synthetic opioids other than methadone (T40.4).
c Jurisdictions with fewer than 20 predicted overdose deaths involving synthetic opioids were excluded, as well as those with suppressed data due to data quality issues.
d Included time periods will have some amount of overlap. For example, the 12-months ending in June 2019 (i.e., July 2018 to June 2019) includes deaths occurring in June 2019, which is also included separately in 12-months ending in May 2020 (i.e., June 2019 to May 2020).
For More Information
- CDC Opioid Overdose homepage: “Understanding the Epidemic”
- CDC Health Advisory: Increases in Fentanyl Drug Confiscations and Fentanyl-related Overdose Fatalities
- CDC Health Advisory: Influx of Fentanyl-laced Counterfeit Pills and Toxic Fentanyl-related Compounds Further Increases Risk of Fentanyl-related Overdose and Fatalities
- CDC Health Advisory: Rising Numbers of Deaths Involving Fentanyl and Fentanyl Analogs, Including Carfentanil, and Increased Usage and Mixing with Non-opioids
References
- Jalal H, Buchanich JM, Roberts MS, Balmert LC, Zhang K, Burke DS. Changing dynamics of the drug overdose epidemic in the United States from 1979 through 2016. Science. 2018 Sep 21;361(6408):eaau1184.
- Wilson N, Kariisa M, Seth P, Smith H IV, Davis NL. Drug and Opioid-Involved Overdose Deaths — United States, 2017–2018. MMWR Morb Mortal Wkly Rep 2020;69:290–297.
- Ahmad FB, Rossen LM, Sutton P. Provisional drug overdose death counts. National Center for Health Statistics. 2020.
- American Medical Association. Issue brief: reports of increases in opioid-related overdose and other concerns during COVID pandemic. Updated December 9, 2020.
- Shover CL, Falasinnu TO, Dwyer CL, et al. Steep increases in fentanyl-related mortality west of the Mississippi River: Recent evidence from county and state surveillance. Drug Alcohol Depend. 2020;216:108314.
- Hedegaard H, Bastian BA, Trinidad JP, Spencer MR, Warner M. Regional differences in the drugs most frequently involved in drug overdose deaths: United States, 2017. National Vital Statistics Reports; vol 68 no 12. Hyattsville, MD: National Center for Health Statistics. 2019.
- O’Donnell J, Gladden RM, Mattson CL, Hunter CT, Davis NL. Vital Signs: Characteristics of Drug Overdose Deaths Involving Opioids and Stimulants — 24 States and the District of Columbia, January–June 2019. MMWR Morb Mortal Wkly Rep 2020;69:1189–1197.
- Drug Enforcement Administration, Diversion Control Division. National Forensic Laboratory Information System: NFLIS-Drug 2019 Midyear Report. 2020. Springfield, VA: U.S. Drug Enforcement Administration.
- Wainwright JJ, Mikre M, Whitley P, Dawson E, Huskey A, Lukowiak A, Giroir BP. Analysis of Drug Test Results Before and After the US Declaration of a National Emergency Concerning the COVID-19 Outbreak. JAMA. 2020 Sep 18;324(16):1674–7.
- Kariisa M, Scholl L, Wilson N, Seth P, Hoots B. Drug overdose deaths involving cocaine and psychostimulants with abuse potential—United States, 2003–2017. MMWR Morb Mortal Wkly Rep 2019;68:388–95.
- Centers for Disease Control and Prevention. HIV Infection, Risk, Prevention, and Testing Behaviors among Persons Who Inject Drugs—National HIV Behavioral Surveillance: Injection Drug Use, 20 U.S. Cities, 2015. HIV Surveillance Special Report 18. Revised edition.
- Drug Enforcement Administration. 2019 National Drug Threat Assessment. Drug Enforcement Administration Strategic Intelligence Section, U.S. Department of Justice. Published December 2019.
- Drug Enforcement Administration, Diversion Control Division. National Forensic Laboratory Information System: NFLIS Drug 2019 Annual Report. Springfield, VA: U.S. Drug Enforcement Administration.
- Jones CM, Olsen EO, O’Donnell J, Mustaquim D. Resurgent Methamphetamine Use at Treatment Admission in the United States, 2008-2017. Am J Public Health. 2020;110(4):509-516.
- Dowell D, Haegerich TM, Chou R. CDC Guideline for Prescribing Opioids for Chronic Pain — United States, 2016. MMWR Recomm Rep 2016;65(No. RR-1):1–49.
- Guy GP Jr., Haegerich TM, Evans ME, Losby JL, Young R, Jones CM. Vital Signs: Pharmacy-Based Naloxone Dispensing — United States, 2012–2018. MMWR Morb Mortal Wkly Rep 2019;68:679–686.
- Wilson CG, Ramage M, Fagan EB. A Primary Care Response to COVID-19 for Patients with an Opioid Use Disorder [published online ahead of print, 2020 Apr 11]. J Rural Health. 2020.
- Bagley SM, Forman LS, Ruiz S, Cranston K, Walley AY. Expanding access to naloxone for family members: The Massachusetts experience. Drug Alcohol Rev. 2018;37(4):480-486.
- Somerville NJ, O’Donnell J, Gladden RM, et al. Characteristics of Fentanyl Overdose — Massachusetts, 2014–2016. MMWR Morb Mortal Wkly Rep 2017;66:382–386.
- Rzasa Lynn R, Galinkin JL. Naloxone dosage for opioid reversal: current evidence and clinical implications. Ther Adv Drug Saf. 2018;9(1):63-88.
- McDonald R, Strang J. Are take-home naloxone programmes effective? Systematic review utilizing application of the Bradford Hill criteria. Addiction. 2016;111(7):1177-1187.
- Townsend T, Blostein F, Doan T, Madson-Olson S, Galecki P, Hutton DW. Cost-effectiveness analysis of alternative naloxone distribution strategies: First responder and lay distribution in the United States. Int J Drug Policy. 2020;75:102536.
- Lambdin BH, Bluthenthal RN, Wenger LD, et al. Overdose Education and Naloxone Distribution Within Syringe Service Programs – United States, 2019. MMWR Morb Mortal Wkly Rep. 2020;69(33):1117-1121. Published 2020 Aug 21.
- Carpenter J, Murray BP, Atti S, Moran TP, Yancey A, Morgan B. Naloxone Dosing After Opioid Overdose in the Era of Illicitly Manufactured Fentanyl. J Med Toxicol. 2020;16(1):41-48.
- Karamouzian M, Kuo M, Crabtree A, Buxton JA. Correlates of seeking emergency medical help in the event of an overdose in British Columbia, Canada: Findings from the Take Home Naloxone program. Int J Drug Policy. 2019;71:157-163.
- Scheuermeyer FX, DeWitt C, Christenson J, et al. Safety of a Brief Emergency Department Observation Protocol for Patients With Presumed Fentanyl Overdose. Ann Emerg Med. 2018;72(1):1-8.e1.
- Binswanger IA, Blatchford PJ, Mueller SR, Stern MF. Mortality after prison release: opioid overdose and other causes of death, risk factors, and time trends from 1999 to 2009. Ann Intern Med. 2013;159(9):592-600.
- Krawczyk N, Mojtabai R, Stuart EA, et al. Opioid agonist treatment and fatal overdose risk in a state-wide US population receiving opioid use disorder services. Addiction. 2020;115(9):1683-1694.
- Klebacher R, Harris MI, Ariyaprakai N, et al. Incidence of Naloxone Redosing in the Age of the New Opioid Epidemic. Prehosp Emerg Care. 2017;21(6):682-687.
- Mattson CL, O’Donnell J, Kariisa M, Seth P, Scholl L, Gladden RM. Opportunities to Prevent Overdose Deaths Involving Prescription and Illicit Opioids, 11 States, July 2016-June 2017. MMWR Morb Mortal Wkly Rep. 2018 Aug 31;67(34):945-951.
- Centers for Medicare & Medicaid Services. Leveraging Existing Health and Disease Management Programs to Provide Mental Health and Substance Use Disorder Resources During the COVID-19 Public Health Emergency.
- Drug Enforcement Administration. Flexibility during the nationwide public health emergency to prescribe buprenorphine.
- Substance Abuse and Mental Health Services Administration (SAMHSA): Opioid Treatment Program (OTP) Guidance.
- Hood JE, Banta-Green CJ, Duchin JS, Breuner J, Dell W, Finegood B, Glick SN, Hamblin M, Holcomb S, Mosse D, Oliphant-Wells T, Shim MM. Engaging an unstably housed population with low-barrier buprenorphine treatment at a syringe services program: Lessons learned from Seattle, Washington. Subst Abus. 2020;41(3):356-364.
- Bachhuber MA, Thompson C, Prybylowski A, Benitez J MSW, Mazzella S MA, Barclay D. Description and outcomes of a buprenorphine maintenance treatment program integrated within Prevention Point Philadelphia, an urban syringe exchange program. Subst Abus. 2018;39(2):167-172.
- Castillo M, Conte B, Hinkes S, Mathre M, NA CJ, Norindr A, Serota DP, Forrest DW, Deshpande AR, Bartholomew TS, Tookes HE. Implementation of a medical student-run telemedicine program for medications for opioid use disorder during the COVID-19 pandemic. Harm Reduct J. 2020;17(1): 88.
- Brooklyn JR, Sigmon SC. Vermont Hub-and-Spoke Model of Care for Opioid Use Disorder: Development, Implementation, and Impact. J Addict Med. 2017 Jul/Aug;11(4):286-292.
- Stoller KB. A collaborative opioid prescribing (CoOP) model linking opioid treatment programs with office-based buprenorphine providers. Addict Sci Clin Pract. 2015;10(Suppl 1):A63.
- Eddie D, Hoffman L, Vilsaint C, Abry A, Bergman B, Hoeppner B, Weinstein C, Kelly JF. Lived Experience in New Models of Care for Substance Use Disorder: A Systematic Review of Peer Recovery Support Services and Recovery Coaching. Front Psychol. 2019 Jun 13;10:1052.
- Winhusen T, Walley A, Fanucchi LC, Hunt T, Lyons M, Lofwall M, Brown JL, Freeman PR, Nunes E, Beers D, Saitz R, Stambaugh L, Oga EA, Herron N, Baker T, Cook CD, Roberts MF, Alford DP, Starrels JL, Chandler RK. The Opioid-overdose Reduction Continuum of Care Approach (ORCCA): Evidence-based practices in the HEALing Communities Study. Drug Alcohol Depend. 2020 Oct 4;217:108325.
- Houry DE, Haegerich TM, Vivolo-Kantor A. Opportunities for Prevention and Intervention of Opioid Overdose in the Emergency Department. Ann Emerg Med. 2018 Jun;71(6):688-690.
- Houry D, Adams J. Emergency Physicians and Opioid Overdoses: A Call to Aid. Ann Emerg Med. 2019 Sep;74(3):436-438.
- Collins SE, Lonczak HS, Clifasefi SL. Seattle’s Law Enforcement Assisted Diversion (LEAD): Program effects on recidivism outcomes. Eval Program Plann. 2017 Oct;64:49-56.
- Mitchell O, Wilson DB, Eggers A, MacKenzie DL. Assessing the effectiveness of drug courts on recidivism: A meta-analytic review of traditional and non-traditional drug courts. J. Crim Justice. 2012;40(1):60-71.
- Vivolo-Kantor AM, Seth P, Gladden RM, et al. Vital Signs: Trends in Emergency Department Visits for Suspected Opioid Overdoses — United States, July 2016–September 2017. MMWR Morb Mortal Wkly Rep 2018;67:279–285.
- Niles JK, Gudin J, Radcliff J, Kaufman HW. The Opioid Epidemic Within the COVID-19 Pandemic: Drug Testing in 2020. Population Health Management. [ahead of print]
- Guerrieri D, Kjellqvist F, Kronstrand R, Gréen H. Validation and Cross-Reactivity Data for Fentanyl Analogs With the Immunalysis Fentanyl ELISA. J Anal Toxicol. 2019 Jan 1;43(1):18-24.
- Graziano S, Anzillotti L, Mannocchi G, Pichini S, Busardò FP. Screening methods for rapid determination of new psychoactive substances (NPS) in conventional and non-conventional biological matrices. J Pharm Biomed Anal. 2019 Jan 30;163:170-179.
- Armenian P, Vo KT, Barr-Walker J, Lynch KL. Fentanyl, fentanyl analogs and novel synthetic opioids: A comprehensive review. Neuropharmacology. 2018 May 15;134(Pt A):121-132.
- Mojica MA, Carter MD, Isenberg SL, Pirkle JL, Hamelin EI, Shaner RL, Seymour C, Sheppard CI, Baldwin GT, Johnson RC. Designing traceable opioid material§ kits to improve laboratory testing during the U.S. opioid overdose crisis. Toxicol Lett. 2019 Dec 15;317:53-58.
- Green TC, Park JN, Gilbert M, McKenzie M, Struth E, Lucas R, Clarke W, Sherman SG. An assessment of the limits of detection, sensitivity and specificity of three devices for public health-based drug checking of fentanyl in street-acquired samples. Int J Drug Policy. 2020 Mar;77:102661.
- Harper L, Powell J, Pijl EM. An overview of forensic drug testing methods and their suitability for harm reduction point-of-care services. Harm Reduct J. 2017 Jul 31;14(1):52.
i Provisional death counts presented in this HAN are the predicted number of deaths for “12-month ending periods,” defined as the number of deaths occurring in the 12-month period ending in the month indicated. For example, the 12-month ending period in June 2019 would include deaths occurring from July 1, 2018, through June 30, 2019; thus, “12-months ending in June 2019” as written indicates deaths spanning July 2018 through June 2019. When analyzing changes in 12-month provisional estimates (e.g., the difference between 12-month ending in June 2019 compared to 12-month ending in May 2020), please consider that differences are driven both by deaths in the new months added to the rolling average (e.g., July 2019 through May 2020) as well as deaths occurring in the month dropped from the rolling count 12-months ago (e.g., July 2018 to May 2019). Predicted provisional counts represent estimates of the number of deaths adjusted for incomplete reporting. Estimates included may differ slightly from final NCHS drug overdose death reports, because provisional data are based on available records that meet certain data quality criteria at the time of analysis and may not include all deaths that occurred during a given time period. Therefore, they should not be considered comparable with final data and are subject to change.
ii It is important to note that the provisional data included in this HAN compares data from 11 months (i.e., data begins in June) rather than the typical 12 months of data that are provided in CDC’s NCHS monthly provisional estimates. Comparisons and percentage change estimates may differ slightly.
iii Regions are defined using Census Regions – Northeast: Connecticut, Maine, Massachusetts, New Hampshire, New Jersey, New York, New York City, Pennsylvania, Rhode Island, and Vermont. Midwest: Illinois, Indiana, Iowa, Kansas, Michigan, Minnesota, Missouri, Nebraska, North Dakota, Ohio, South Dakota, and Wisconsin. South: Alabama, Arkansas, Delaware, District of Columbia, Florida, Georgia, Kentucky, Louisiana, Maryland, Mississippi, North Carolina, Oklahoma, South Carolina, Tennessee, Texas, Virginia, and West Virginia. West: Alaska, Arizona, California, Colorado, Hawaii, Idaho, Montana, Nevada, New Mexico, Oregon, Utah, Washington, and Wyoming.
The Centers for Disease Control and Prevention (CDC) protects people’s health and safety by preventing and controlling diseases and injuries; enhances health decisions by providing credible information on critical health issues; and promotes healthy living through strong partnerships with local, national and international organizations.
Department of Health and Human Services
HAN Message Types
- Health Alert: Conveys the highest level of importance about a public health incident.
- Health Advisory: Provides important information about a public health incident.
- Health Update: Provides updated information about a public health incident.
###
This message was distributed to state and local health officers, state and local epidemiologists, state and local laboratory directors, public information officers, HAN coordinators, and clinician organizations.
###