Update and Interim Guidance on Outbreak of 2019 Novel Coronavirus (2019-nCoV)

Distributed via the CDC Health Alert Network
February 1, 2020, 0900 ET (9:00 AM ET)
CDCHAN-00427
Summary
The Centers for Disease Control and Prevention (CDC) continues to closely monitor an outbreak of respiratory illness caused by a novel coronavirus (2019-nCoV) that was initially detected in Wuhan City, Hubei Province, China in December 2019.
This CDC Health Alert Network (HAN) Update provides a situational update and interim guidance to state and local health departments that supersedes guidance in CDC’s HAN 426 distributed on January 17, 2020. It also adds
- guidance for clinicians caring for patients with 2019-nCoV (https://www.cdc.gov/coronavirus/2019-ncov/hcp/clinical-guidance-management-patients.html),
- and for public health officials on the evaluation and testing of patients under investigation (PUIs) for 2019-nCoV (https://www.cdc.gov/coronavirus/2019-nCoV/hcp/clinical-criteria.html), and
- updated infection prevention and control guidance specific to 2019-nCoV (https://www.cdc.gov/coronavirus/2019-nCoV/hcp/infection-control.html).
Early in the outbreak, many of the patients with respiratory illness caused by 2019-nCoV in China had exposure to a large seafood and live animal market, suggesting animal-to-human transmission. More recently, cases have been confirmed with no exposure to animal markets, indicating that person-to-person spread of the virus has occurred. Chinese officials report that sustained person-to-person spread in the community is occurring in China.
The first US case-patient was identified on January 21, 2020, and had recently traveled from Wuhan, China. Since that time, six additional cases have been confirmed in the United States, four among persons who traveled from Wuhan, and one a close contact of a confirmed case. Globally, reported illnesses in people with 2019-nCoV have ranged from mild (no or few signs and symptoms), to severe, including death. These findings are consistent with other coronaviruses, including Severe Acute Respiratory Syndrome (SARS) (https://www.cdc.gov/sars/) and Middle East Respiratory Syndrome (MERS) (https://www.cdc.gov/coronavirus/mers/index.html). Additional information about 2019-nCoV is needed to better understand transmission, disease severity, and risk to the general population. The goal of the ongoing US public health response is to identify and contain this outbreak and prevent sustained spread of 2019-nCoV in the United States.
Recommendations for Screening of Patients for 2019-nCoV in Healthcare Facilities
Recommendations for screening of patients for possible 2019-nCoV infection are based on (1) current knowledge of the characteristics of clinical illness observed in early cases, and (2) the geographic distribution of current cases. They reflect the current public health goal of rapidly containing and preventing transmission of 2019-nCoV illness.
Patients presenting to healthcare facilities should be assessed for exposures associated with risk of 2019-nCoV infections (e.g., travel to China or close contact with a confirmed case) and for symptoms consistent with 2019-nCoV infection (https://www.cdc.gov/coronavirus/2019-nCoV/hcp/clinical-criteria.html). The assessment is intended to allow healthcare providers to make decisions about appropriate infection control and management of patients. Note that the signs and symptoms of 2019-nCoV overlap with those associated with other viral respiratory tract infections. Given the time of year, common respiratory illnesses, including influenza, should also be considered in patients who are screened. (Figure 1)
Clinicians should ask:
- Does the person have fever or symptoms of lower respiratory infection, such as cough or shortness of breath?
AND
- Has the patient traveled to mainland China within 14 days of symptom onset?
OR
- Has the patient had close contact1 with a person confirmed with 2019-nCoV infection?
Figure 1.
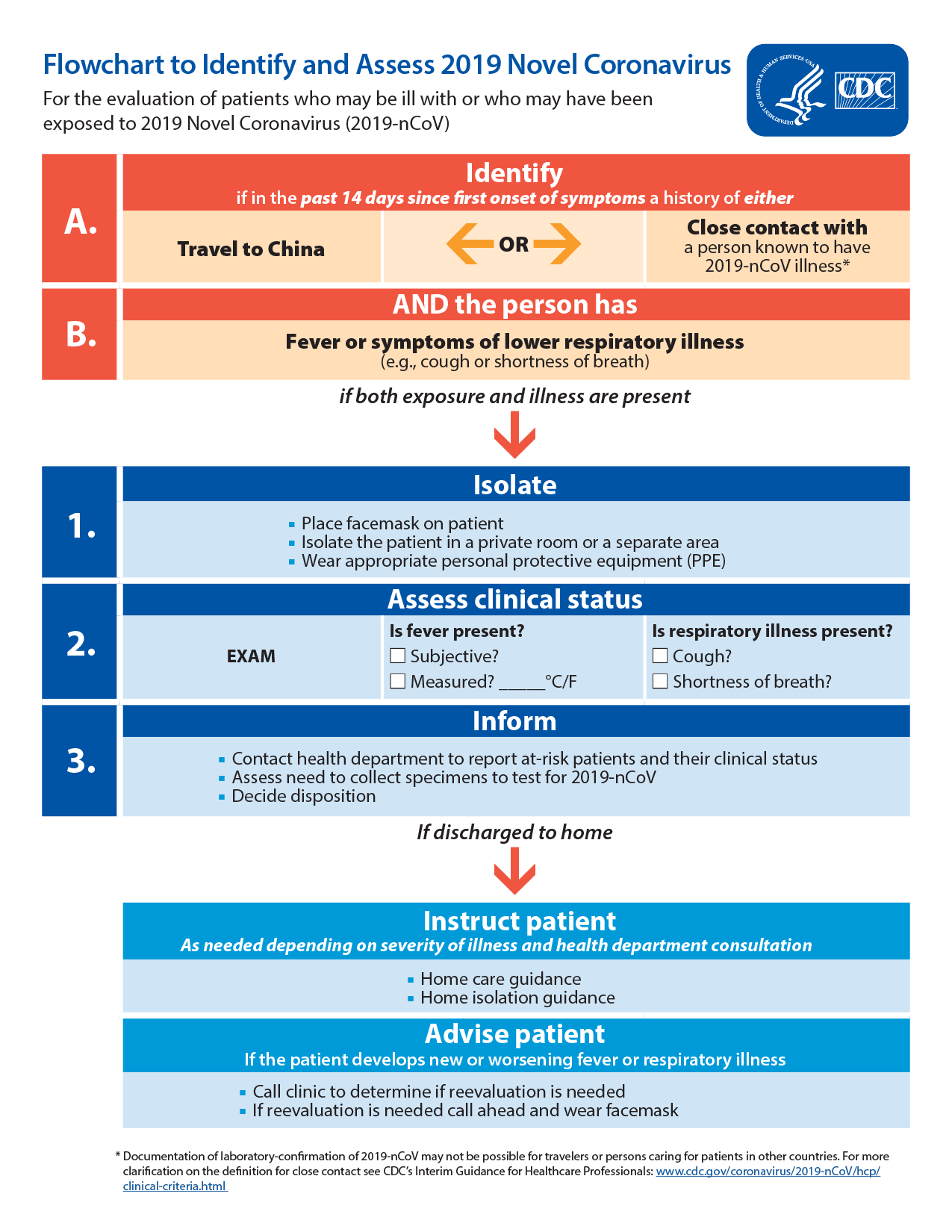
If a patient meets these criteria:
- To minimize the risk that other people will be exposed to individuals who may have 2019-nCoV, patients who report having these symptoms should be asked to wear a surgical mask as soon as they are identified and directed to a separate area, if possible, with at least 6 feet (2 meters) separation from other persons. Patients should be evaluated in a private room with the door closed, ideally an airborne infection isolation room (AIIR), if available. Healthcare personnel entering the room should use standard precautions, contact precautions, airborne precautions, and use eye protection (e.g., goggles or a face shield). For more information about this, see CDC’s Interim Infection Prevention and Control Recommendations for Patients with Known or Patients Under Investigation for 2019 Novel Coronavirus (2019-nCoV) in a Healthcare Setting (https://www.cdc.gov/coronavirus/2019-nCoV/hcp/infection-control.html).
Clinicians should immediately notify the healthcare facility’s infection control personnel and local health department. The health department will determine if this patient needs to be considered a PUI for 2019-nCoV and be tested for infection.
Criteria to Guide Evaluation and Testing of Patients Under Investigation (PUI) for 2019-nCoV
Local health departments, in consultation with clinicians, should determine whether a patient is a PUI for 2019-nCoV. The CDC clinical criteria for 2019-nCoV PUIs have been developed based on available information about this novel virus, as well as what is known about SARS and MERS. These criteria are subject to change as additional information becomes available.
These criteria are intended to serve as guidance for evaluation and testing. Patients should be evaluated and discussed with public health departments on a case-by-case basis for possible 2019-nCoV infection. Testing decisions might be further informed by the clinical presentation or exposure history (e.g., uncertain travel or exposure), and the presence of an alternative diagnosis that explains their clinical presentation.
Recommendations for Reporting, Testing, and Specimen Collection
Healthcare providers should immediately notify infection control personnel at their healthcare facility if a patient is classified a PUI for 2019-nCoV. State health departments that have identified a PUI should immediately contact CDC’s Emergency Operations Center (EOC) at 770-488-7100 and complete a 2019-nCoV PUI case investigation form (https://www.cdc.gov/coronavirus/2019-ncov/hcp/clinical-criteria.html#reporting-testing-specimen-collection). CDC’s EOC will assist local and state health departments with obtaining, storing, and shipping appropriate specimens to CDC, including afterhours or on weekends or holidays. Currently, diagnostic testing for 2019-nCoV can be done only at CDC. Testing for other respiratory pathogens should not delay specimen shipping to CDC.
For initial diagnostic testing for 2019-nCoV, CDC recommends collecting and testing upper respiratory (nasopharyngeal AND oropharyngeal swabs), and lower respiratory (sputum, if possible)) for those patients with productive coughs. Induction of sputum is not indicated. Specimens should be collected as soon as possible once a PUI is identified, regardless of the time of symptom onset. See Interim Guidelines for Collecting, Handling, and Testing Clinical Specimens from Patients Under Investigation (PUIs) for 2019 Novel Coronavirus (2019-nCoV) (https://www.cdc.gov/coronavirus/2019-nCoV/lab/guidelines-clinical-specimens.html).
Recommendations for Healthcare Providers
No vaccine or specific treatment for 2019-nCoV infection is available. At present, medical care for patients with 2019-nCoV is supportive.
Persons with confirmed or suspected 2019-nCoV infection who are hospitalized should be evaluated and cared for in a private room with the door closed, ideally an airborne infection isolation room, if available. For more information, see Interim Infection Prevention and Control Recommendations for Patients with Known or Patients Under Investigation for 2019 Novel Coronavirus (2019-nCoV) in a Healthcare Setting (https://www.cdc.gov/coronavirus/2019-nCoV/hcp/infection-control.html).
Home care and isolation may be an option, based on clinical and public health assessment, for some persons. Please see Interim Guidance for Preventing the Spread of 2019 Novel Coronavirus (2019-nCoV) in Homes and Communities (https://www.cdc.gov/coronavirus/2019-ncov/hcp/guidance-prevent-spread.html).
Those isolated at home should be monitored by public health officials to the extent possible. Refer to Interim Guidance for Implementing Home Care of People Not Requiring Hospitalization for 2019 Novel Coronavirus (2019-nCoV) (https://www.cdc.gov/coronavirus/2019-ncov/hcp/guidance-home-care.html) for more information.
Notes
1Close contact is defined as:
a) being within approximately 6 feet (2 meters), or within the room or care area, of a 2019-nCoV case for a prolonged period of time while not wearing recommended personal protective equipment or PPE (e.g., gowns, gloves, NIOSH-certified disposable N95 respirator, eye protection); close contact can include caring for, living with, visiting, or sharing a health care waiting area or room with a 2019-nCoV case
– or –
b) having direct contact with infectious secretions of a 2019-nCoV case (e.g., being coughed on) while not wearing recommended personal protective equipment.
2Fever may be subjective or confirmed
See CDC’s updated Interim Infection Prevention and Control Recommendations for Patients with Known or Patients Under Investigation for 2019 Novel Coronavirus (2019-nCoV) in a Healthcare Setting (https://www.cdc.gov/coronavirus/2019-ncov/infection-control.html).
Data to inform the definition of close contact are limited. Considerations when assessing close contact include the duration of exposure (e.g., longer exposure time likely increases exposure risk) and the clinical symptoms of the person with 2019-nCoV (e.g., coughing likely increases exposure risk as does exposure to a severely ill patient). Special consideration should be given to those exposed in health care settings.
3 Documentation of laboratory-confirmation of 2019-nCoV may not be possible for travelers or persons caring for patients in other countries.
4 Category also includes any member of a cluster of patients with severe acute lower respiratory illness (e.g., pneumonia, ARDS) of unknown etiology in which 2019-nCoV is being considered that requires hospitalization. Such persons should be evaluated in consultation with state and local health departments regardless of travel history.
For More Information
More information is available at the 2019 Novel Coronavirus website (https://www.cdc.gov/coronavirus/2019-ncov/index.html) or by
calling 800-CDC-INFO | (800-232-4636) | TTY: (888) 232-6348
The Centers for Disease Control and Prevention (CDC) protects people’s health and safety by preventing and controlling diseases and injuries; enhances health decisions by providing credible information on critical health issues; and promotes healthy living through strong partnerships with local, national and international organizations.
Department of Health and Human Services
HAN Message Types
- Health Alert: Conveys the highest level of importance about a public health incident.
- Health Advisory: Provides important information about a public health incident.
- Health Update: Provides updated information about a public health incident.
###
This message was distributed to state and local health officers, state and local epidemiologists, state and local laboratory directors, public information officers, HAN coordinators, and clinician organizations.
###