Ebola Report: Strengthening Health Care and Preventing Infections
About CDC
‹View Table of Contents

Lindsey Horton, CDC responder, demonstrates how to clean up infected body fluids at an Ebola treatment unit in Guinea.

The inside of a mock Ebola treatment unit at CDC’s training course for healthcare workers in Anniston, Alabama.
Effective infection control can protect communities and the healthcare workers who serve them. Before the Ebola outbreak, infection control in health facilities in Guinea, Liberia, and Sierra Leone was often minimal at best. Fragile healthcare systems added to the rapid spread of the virus and made it difficult to contain the epidemic. In addition, community behaviors needed to change to keep people from getting Ebola when caring for people who were sick or participating in traditional burials. Responders on the ground in West Africa have been working closely with partners and the ministries of health to provide training and health education to reduce the spread of disease. In addition to training, CDC and partners hosted innovative microplanning sessions in Liberia, which focused on early detection and safe isolation of patients, safe burials, and infection control in healthcare settings.
When the first case of Ebola was diagnosed in the United States, CDC worked to tighten infection control procedures. We used the knowledge gained from managing this case to improve preparation of healthcare workers and hospitals around the country.
“We simulated triage of people with unknown Ebola status, putting on and taking off authentic ETU protective equipment, drawing blood from a patient with confirmed Ebola, transporting a body to the morgue, and cleaning up contaminated body fluids.”
— Kim Newsome, instructor at training course, Anniston, Alabama
Stories from the Field

A group of students evaluates how to move a “patient” into the mock ETU at CDC’s training course in Anniston, Alabama.
The mock Ebola treatment unit (ETU) was a sparse, low-technology space that contrasted sharply with the high technology protective equipment ETU workers must wear every day. Bright yellow suits, orange plastic dividers, hospital cots, and antiseptic sprayers filled the unit, copying every detail of the West African ETUs where volunteer clinicians work. From the hand washing station at the entrance to the station where personal protective equipment is removed, the simulated unit made Kim Newsome feel as if she had been transported to another place.
Kim left a desk job at CDC where data and research drives her day, and the effects of her work are several steps removed. In Anniston, the purpose of her work had a face—the ETU volunteer who would soon be traveling to West Africa. As an instructor, Kim’s goal was to provide mock experiences that a real ETU worker might face every day.
During exercises, most trainers met the students in the same way a patient in the ETU would see them—dressed in full protective gear. Staring into the goggled and sometimes anxious eyes of soon-to-be ETU clinicians brought the purpose of their work into sharp focus. The trainers were driven by a common goal of providing lifesaving information for people traveling to West Africa to care for patients there.

A staff member rests outside an Ebola treatment unit.
Kwan Kew Lai, a graduate of CDC’s training course in Anniston, Alabama, served as a doctor with the International Medical Corps in an ETU in Liberia. She knew the work was going to be dangerous, but she also knew her skills were desperately needed.
Each day, Kwan Kew had to use her training, meticulously donning and doffing her PPE, a process that took 15 to 20 minutes each time. Even with temperatures reaching 89°F during training in Alabama, those conditions were nothing like the humid weather the trainees would face in West Africa.
The physical demands, weather, and hot gear worn in the ETU were not the only challenges Kwan Kew faced. It was hard for her to care for patients and encourage them to be hopeful while being encumbered by PPE.
“What makes it even more poignant is that when the patients need close human contact the most, in times of extreme suffering, pain, and fear, there is none to offer except with a barrier of protective covering,” she said. “In the beginning, it hit home to me that there was a real possibility of a true exposure; however, as time went on, inspired by the persistence, dedication, and selfless caring of my colleagues, that fear was pushed to the back of my mind and the goal of getting the patients better overwhelmingly became my main concern.”

Close to 250 people showed up for the first day of Heidi Soeters’ and Lindsey Horton’s training.
When thinking about infection control in Guinea, it’s helpful to picture the average health facility in that country. It’s usually one to two rooms, it doesn’t have electricity or running water, and it’s crowded with sick patients.
Heidi Soeters and Lindsey Horton, both CDC responders, implemented an infection control training course for Guinean healthcare workers.
“Our infection control program trains frontline healthcare workers, everyone from doctors and nurses to janitors and ambulance drivers. The training included hands-on exercises in hand washing, triage of patients, putting on protective equipment, and cleaning up contaminated fluids,” Lindsey said.
Heidi and Lindsey served as technical advisors for the training sponsor, Catholic Relief Services. Students were recruited from nearby health facilities, but on the first day of training, people came from as far as 25 miles away.
“On the first day of the course, we had 80 students enrolled, but more than 100 more showed up eager to be trained and begging to have a spot in the course. Fortunately, we were able to add more sessions to cover all healthcare workers in three priority regions of Guinea,” Lindsey said. “These efforts have the added benefit of being important not just in the context of an Ebola epidemic, but also because they are creating lasting improvements in infection control that should be there for years to come.”
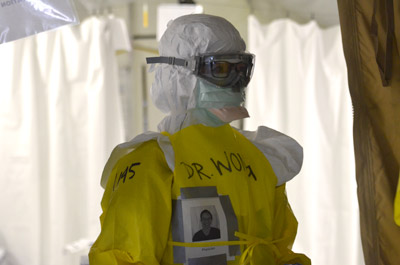
Karen Wong ready to admit a patient at the Monrovia Medical Unit in Monrovia.
Channeling the mentality of a scuba diver helped Karen Wong work safely and effectively inside an ETU. Karen was part of the first team deployed to work at the Monrovia Medical Unit in Liberia. “Once you put your personal protective equipment on, your countdown starts in terms of how long you’re able to stay in there comfortably,” she explained. Like a diver underwater, she needed to go into the ETU with a dive plan. “It’s important to figure out what everyone needed to do before entering the ETU,” she added.
Karen did not dive head first into the ETU. “Part of what let me keep going with doing this kind of scary, high risk work was knowing that I had been trained really well in keeping myself safe.” She was one of the 650 healthcare workers who participated in the 3-day training course in Anniston, Alabama, that taught medical professionals about personal protective equipment, how to use it, and how to stay safe as they administered care to patients with Ebola.
“One thing they really focused on during training was our personal safety. If you compromise your safety while treating your first patient, you won’t be able to help the next one,” said Karen.

Burial team buries an Ebola victim in Sierra Leone.
One thing that comes with an outbreak is a need to bury bodies. With Ebola, this cannot be done casually because corpses are the most infectious thing out there. “If you come into contact with the dead body of an Ebola victim, you are very likely to get Ebola yourself. Therefore, people need to be specifically trained on how to bury bodies of people who died from Ebola,” said Leisha Nolen, CDC responder. They are trained how to put on protective suites, masks, goggles, and gloves; how to collect bodies; how to wrap the corpses; and how to bury them. Keep in mind, the people on burial teams usually work on farms or building houses—burying bodies is not their usual job, so all of this is as terrible to them as it would be to you. And it turns out that the obvious part of their job, putting on the equipment and burying the bodies, is not the most difficult part of their job. Instead, it is the part no one expected that is the hardest: the part where the teams have to convince families that taking their loved one to be buried is the right thing to do. In Sierra Leone, washing and burying the dead is an important part of honoring their family.
“Burial teams told me over and over how they had to sit and talk to families for hours before the family would let them take the corpse away for safe burial,” Leisha explained. “And they would sit and talk for hours just to make a family understand why it was helping the whole community to allow their loved one to be buried without the usual ritual.”

John Brooks was the lead of CDC’s Ebola Medical Care Task Force in September - October 2014 and March 2015.
During the response, John Brooks, lead for CDC’s Ebola Response Medical Care Task Force, was responsible for teaching U.S. doctors, nurses, and the general public about how Ebola spreads and how to prevent infection. He and his team led dozens of calls with hospitals on the science behind Ebola and taught them how to evaluate patients reporting symptoms of the virus.
“It was a hectic time. The public had been seized with fear of Ebola, and we were doing our best to manage that fear with science-based information,” said John.
“I learned a powerful lesson during my Ebola work, and that is the power of fear. Fear is a natural emotion; it’s supposed to protect us from injury or infection. When you see that lion, you run! But too much fear can be a bad thing. It was our responsibility to understand the science behind Ebola and use that to encourage positive action, not panic,” he said.
“To understand an epidemic, you often need the 35,000-foot view, looking for trends and patterns,” John said. “But you also need to find out what’s going on at ground level, what’s happening to the people at risk of, and being affected by, the condition you’re trying to prevent.”

Healthcare workers practice providing care for a patient with Ebola in a mock scenario.
One of the ways CDC helped to prepare U.S. hospitals for a possible patient with Ebola was by sending teams of CDC experts in infection prevention and control, occupational health, and diagnostic laboratory practices—called Rapid Ebola Preparedness (REP) teams—to 81 facilities in 21 states and Washington, DC, to assess their readiness for caring for patients with Ebola. Ron Hall, an Ebola responder based in CDC’s National Institute for Occupational Safety and Health, was part of one of these REP teams. He visited U.S. hospitals to evaluate their readiness to safely care for a patient with Ebola. “You’re working in hospitals versus a disaster site, but from an occupational safety and health point of view, we’re still looking out for the workers, which are healthcare workers,” he said.
REP teams were composed of 4 to 10 CDC experts in infection control, occupational health, and laboratory issues, as well as external local experts. According to Ron, “this holistic approach was very important in helping these hospitals achieve what they need to achieve: taking care of patients with Ebola safely and efficiently without getting anyone else sick.”
The United States has expanded its network of hospitals prepared and certified to treat Ebola patients, increasing capacity from just three facilities to 55 facilities in 17 states and Washington, DC.

Brian Christiansen, CDC Infection Control Team (left), at an Ebola educational session or healthcare workers at the Jacob Javits Center in New York in October 2014.
When the first case of Ebola was diagnosed in the United States, and two nurses became infected with the disease, a group at CDC worked quickly to create training on personal protective equipment for healthcare workers in the United States.
CDC worked with a diverse group of partners to provide Ebola infection control training to U.S. healthcare workers through a multifaceted approach. CDC and partners worked together to provide U.S. healthcare workers with the information they needed through web-based tools, daily calls, mobile-friendly training applications, live training events, and in-depth clinical trainings by experts at Emory University Hospital and Nebraska Medical Center. With strategic partners, CDC was able to reach more than 150,000 healthcare workers.
CDC also partnered with Partnership for Quality Care and healthcare unions to conduct live training events in New York City, Los Angeles, and Philadelphia, reaching more than 6,500 people in-person, and more than 20,000 via live webcast. Additionally, CDC, Emory University Hospital, and Nebraska Medical Center trained more than 460 healthcare workers from 87 healthcare systems, including 37 new Ebola treatment centers, on all aspects of infection control and care for patients with Ebola.
Table of Contents
- The Road to Zero
- Introduction
- Tracing Contacts
- ›Strengthening Health Care and Preventing Infections
- Mobilizing Laboratories
- Protecting Borders
- Communicating and Educating
- Overcoming Challenges
- Moving Forward
- Timeline
- Ebola by the Numbers