Recommendations for Fully Vaccinated People
COVID-19 Homepage
Strategies for Optimizing the Supply of N95 Respirators
Situational update as of May 2021: The supply and availability of NIOSH-approved respirators have increased significantly over the last several months. Healthcare facilities should not be using crisis capacity strategies at this time and should promptly resume conventional practices. Check the NIOSH Certified Equipment List to identify all NIOSH-approved respirators.
Healthcare facilities should stop purchasing non-NIOSH-approved respirators for use as respiratory protection and consider using any that have been stored for source control where respiratory protection is not needed. Respirators that were previously used and decontaminated should not be stored. We do not know the long-term stability of non-NIOSH-approved respirators and respirators that have been decontaminated, and if these will be recommended for use in the future. Healthcare facilities should return to using only NIOSH-approved respirators where needed.
Summary of Recent Changes
Audience: These considerations are intended for use by federal, state, and local public health officials, respiratory protection program managers, leaders in occupational health services and infection prevention and control programs, and other leaders in healthcare settings who are responsible for developing and implementing policies and procedures for preventing pathogen transmission in healthcare settings.
Purpose: This document offers a series of strategies or options to optimize supplies of disposable N95 filtering facepiece respirators (commonly called “N95 respirators”) in healthcare settings when there is limited supply. It does not address other aspects of pandemic planning; for those, healthcare facilities can refer to COVID-19 preparedness plans. The strategies are also listed in order of priority and preference in the Summary for Healthcare Facilities: Strategies for Optimizing the Supply of N95 Respirators during the COVID-19 Response in an easy-to-use format for healthcare facilities.
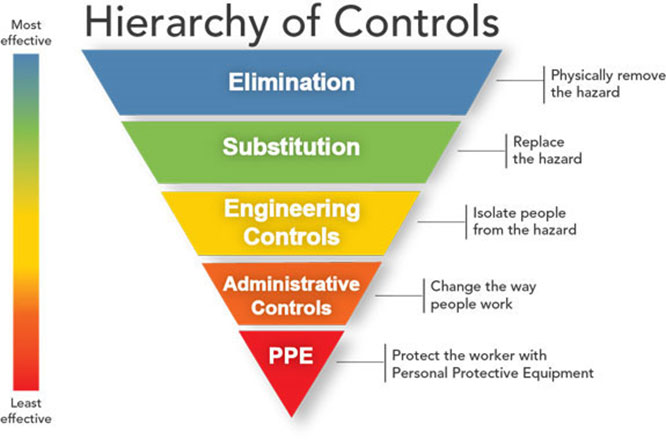
Controlling exposures to occupational hazards is a fundamental way to protect personnel. Conventionally, a hierarchy has been used to achieve feasible and effective controls. Multiple control strategies can be implemented concurrently or sequentially. This hierarchy can be represented as follows:
- Elimination
- Substitution
- Engineering controls
- Administrative controls
- Personal protective equipment (PPE)
To prevent infectious disease transmission, elimination (physically removing the hazard) and substitution (replacing the hazard) are not typically options for healthcare settings. However, exposures to transmissible respiratory pathogens in healthcare facilities can often be reduced or possibly avoided through engineering and administrative controls and PPE. Prompt detection and effective triage and isolation of potentially infectious patients are essential to prevent unnecessary exposures among patients, healthcare personnel (HCP), and visitors at the facility.
N95 respirators are the PPE most often used to control exposures to infectious pathogens transmitted via the airborne route, though their effectiveness is highly dependent upon proper fit and use. N95 respirators are intended to be used once and then properly disposed of and replaced with a new N95 respirator. The optimal way to prevent airborne transmission is to use a combination of interventions from across the hierarchy of controls, not just PPE alone. Applying a combination of controls can provide an additional degree of protection, even if one intervention fails or is not available.
Respirators, when required to protect HCP from airborne contaminants such as some infectious agents, must be used in the context of a comprehensive, written respiratory protection program that meets the requirements of Occupational Safety and Health Administration (OSHA) Respiratory Protection standard. The program should include medical evaluations, training, and fit testing.
Surge capacity refers to the ability to manage a sudden increase in patient volume that would severely challenge or exceed the present capacity of a facility. While there are no commonly accepted measurements or triggers to distinguish surge capacity from daily patient care capacity, surge capacity is a useful framework to approach a decreased supply of N95 respirators during the COVID-19 response. To help healthcare facilities plan and optimize the use of respiratory protection in response to COVID-19, CDC has developed a Personal Protective Equipment (PPE) Burn Rate Calculator. Three general strata have been used to describe surge capacity and can be used to prioritize measures to conserve N95 respirator supplies along the continuum of care.1
- Conventional capacity: measures consisting of engineering, administrative, and PPE controls should already be implemented in general infection prevention and control plans in healthcare settings.
- Contingency capacity: measures that may be used temporarily during periods of expected N95 respirator shortages. Contingency capacity strategies should only be implemented after considering and implementing conventional capacity strategies. While current supply may meet the facility’s current or anticipated utilization rate, there may be uncertainty if future supply will be adequate and therefore, contingency capacity strategies may be needed.
- Crisis capacity: strategies that are not commensurate with U.S. standards of care but may need to be considered during periods of known N95 respirator shortages. Crisis capacity strategies should only be implemented after considering and implementing conventional and contingency capacity strategies. Facilities can consider crisis capacity when the supply is not able to meet the facility’s current or anticipated utilization rate.
CDC’s optimization strategies for N95 respirator supply offer a continuum of options for use when PPE supplies are stressed, running low, or exhausted. Contingency and then crisis capacity measures augment conventional capacity measures and are meant to be considered and implemented sequentially. Once N95 respirator availability returns to normal, healthcare facilities should promptly resume conventional practices.
Decisions to implement contingency and crisis strategies are based upon these assumptions:
- Facilities understand their NIOSH-approved respirator inventory and supply chain
- Facilities understand their NIOSH-approved respirator utilization rate
- Facilities are in communication with local healthcare coalitions and federal, state, and local public health partners (e.g., public health emergency preparedness and response staff) to identify additional supplies
- Facilities have already implemented other engineering and administrative control measures including:
- Use physical barriers and other engineering controls
- Limit number of patients going to hospital or outpatient settings
- Use telemedicine whenever possible
- Limit all HCP not directly involved in patient care
- Limit face-to-face HCP encounters with patients
- Limit visitors to the facility to those essential for the patient’s physical or emotional well-being and care (e.g., care partner, parent)
- Cohort patients and/or HCP
- Facilities have provided HCP with required education and training, including having them demonstrate competency with donning and doffing, with any PPE ensemble that is used to perform job responsibilities, such as provision of patient care
Once availability of NIOSH-approved respirators returns to normal, healthcare facilities should promptly resume conventional practices. Determining the appropriate time to return to conventional strategies can be challenging. Considerations affecting this decision include:
- The number of patients for whom respirator use is recommended for their care (e.g., number of patients with suspected or confirmed SARS-CoV-2 infection)
- Whether there is evidence of ongoing SARS-CoV-2 transmission in the facility
- The incidence of COVID-19 in the community
- The number of days’ supply of respirators currently remaining at the facility
- Whether or not the facility is receiving regular resupply with its full allotment
Engineering Controls
Engineering controls reduce exposures for HCP by placing a barrier between the hazard and the HCP. Engineering controls can be very effective as part of a suite of strategies to protect HCP without placing primary responsibility of implementation on them (i.e., they function without HCP having to take an action).
Administrative Controls
Administrative controls are employer-dictated work practices and policies that reduce or prevent hazardous exposures. Their effectiveness depends on employer commitment and HCP acceptance and consistent use of the strategies.
Personal Protective Equipment: Respiratory Protection
While engineering and administrative controls should be considered first when selecting controls, the use of personal protective equipment (PPE) should also be part of a suite of strategies used to protect personnel. Proper use of respiratory protection by HCP requires a comprehensive program (including medical clearance, training, and fit testing) that complies with OSHA’s Respiratory Protection Standard and a high level of HCP involvement and commitment. The program should also include provisions for the cleaning, disinfecting, inspection, repair, and storage of respirators used by HCP on the job according to manufacturer’s instructions. Proper storage conditions can maximize shelf life of respirators. The following strategies in this section are traditionally used by some healthcare systems. If not already implemented, these strategies can be considered by healthcare settings in the face of a potential N95 respirator shortage before implementing the contingency strategies that are listed further below.
Administrative Controls
Personal Protective Equipment: Respiratory Protection
References
- 1 Hick JL, Barbera JA, Kelen GD. Refining surge capacity: conventional, contingency, and crisis capacity. Disaster Med Public Health Prep. 2009;3(2 Suppl): S59-67.
- 2 Fisher EM and Shaffer RE. Considerations for recommending extended use and limited reuse of filtering facepiece respirators in health care settings. J Occup Env Hygiene. 2014; 11(8): D115-D128.
- 3 Bergman, MS, Viscusi DJ, Zhuang Z, Palmiero AJ, Powell JB, Shaffer RE. Impact of multiple consecutive donnings on filtering facepiece respirator fit. Am J Infect Control. 2012;40(4): 375-380.
- 4 van Doremalen N, Bushmaker T, Morris DH. Aerosol and Surface Stability of SARS-CoV-2 as Compared with SARS-CoV-1. N Engl J Med. 2020 Mar 17.